From Workaround to Concept: The Spark
The fall of Roe v. Wade in the United States in 2022, which removed federal abortion rights, created major challenges for patients served by health centers affiliated with Planned Parenthood of America (PPFA).[1] State-level restrictions disrupted patient-provider connections, and the lingering effects of the COVID-19 pandemic reinforced the urgency of telehealth solutions. By late 2022, PPFA’s Digital Strategy (DS) team sought to ease the burden of long-distance travel for patients in states with abortion restrictions and to reduce confusion navigating complex state laws.
Health-center staff were constrained by a cumbersome online appointment scheduling (OAS) system with limited functionality and a rigid website layout. This restricted the range of services they could offer digitally. Many health centers were already listing telehealth schedules separately from in-person services, but national tools were not evolving to meet these needs. Meanwhile, demand for abortion services increased. Data from the #WeCount data project shows that there were 1.14 million abortions in 2024, an increase from 1.05 million abortions in 2023.[2] Direct-to-patient medication abortion (DTP MAB) – the delivery of abortion pills following a telehealth consultation – became a time-sensitive option that more patients and providers explored due to gestational age limits.
Recognizing these challenges, several product and design leads on the DS team collaborated to define, test, and build a new way of elevating existing telehealth services. Our work spanned appointment scheduling, search tools, zip code management, and the database overseeing over 500 health centers nationwide. Navigating an organization historically rooted in brick-and-mortar care, we encountered multiple layers of administration. With limited guidance from leadership, we bypassed standard protocols and made decisions outside typical software and decision-making structures. This is consistent with similar patterns in the health care industry, where organizations that prioritize innovation during crisis outperform their peers during the recovery period (McKinsey & Company 2020).
In organizational theory, “tact” describes decision-making under high uncertainty and extreme pressure. This environment created the conditions for tact to unfold (Kornberger 2019). Our user-first mindset exposed heartbreaking stories of patients losing access to care in states with abortion restrictions. Providers wanted to continue offering care but faced legal and systemic barriers. Amidst the growing legal constraints, our team shifted to a bolder, more flexible product and research cadence, working beyond our usual protocols and stepping outside our standard processes and structures.
Each of PPFA associated affiliates had staff responsible for updating online health center information. Roles varied – from marketing to appointment scheduling – but all were committed to serving patients and highlighting available services. As scheduling and health care needs evolved, these administrators developed workarounds to display the full extent of services despite limitations in national tools. This often resulted in inconsistent formatting, text-heavy pages, and conflicting information.
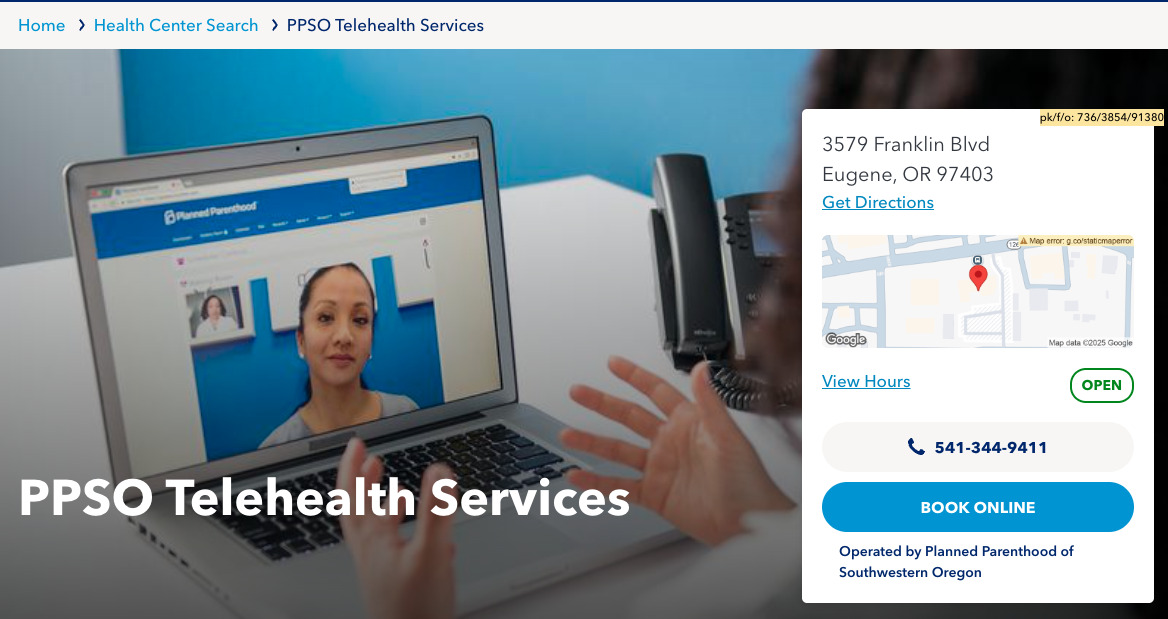
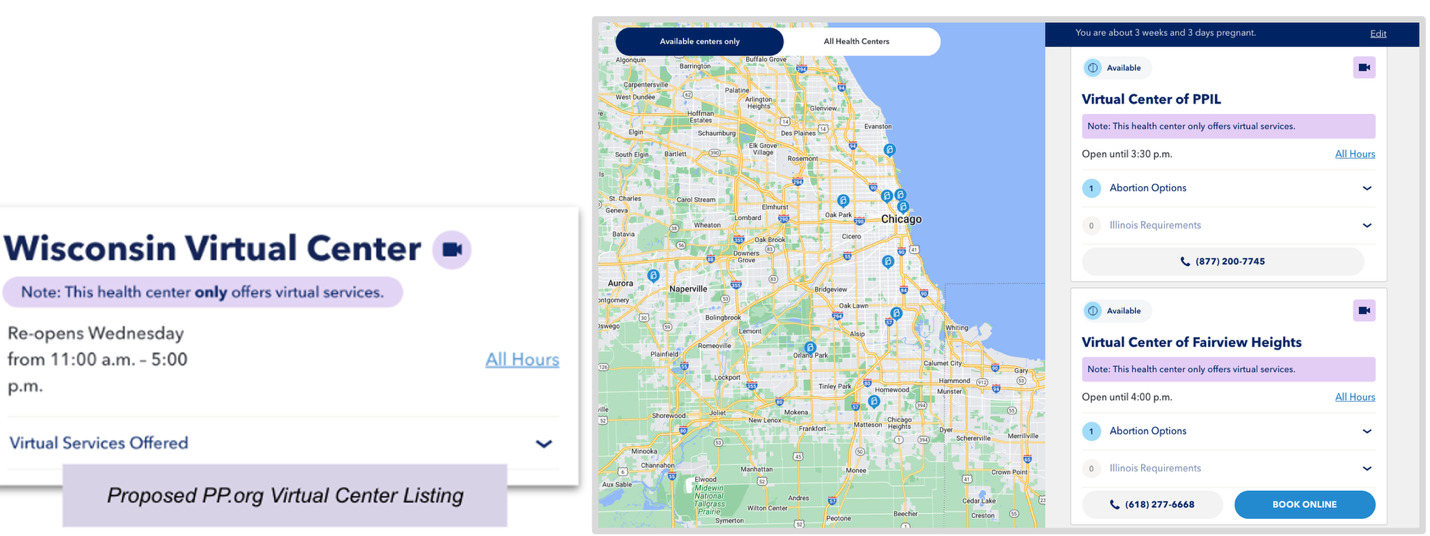
One workaround stood out: Some affiliates transformed a brick-and-mortar health center page into one that listed strictly telehealth services, aiming to improve user access and circumvent scheduling limitations. Internally, this workaround became known as a “fake health center” (Fig.1) because it did not follow the standard organizational model. Inspired by this ingenuity, we asked: what if we built a high-quality, scalable telehealth-only model, fully supported by the scheduling database, instead of relying on ad-hoc workarounds? This idea evolved into Virtual Health Centers (VHCs).
As of September 2025, the experimentation and resourcefulness of health center staff led to the creation of 44 VHCs operating in 37 states, supported by 27 affiliates and collectively serving thousands of patients. VHCs have also mitigated the impact of physical health center closures over the past two years.
Pilot Design and Methodology
This study unfolded in three iterative phases, beginning with a lean, rapid-response effort shaped by the escalating abortion-access crisis.
Phase 1 – validated abortion-first flow. It centered on a focused pilot. We partnered with health-center operations managers and clinicians through workshops and interviews, refining the virtual-clinic interface to prioritize abortion services. We also ran usability studies to understand how patients and staff navigated our designs.
Phase 2 – full-service listing viability. It broadened the product to support all telehealth services and onboarded a select group of additional affiliates. Regional operators were eager to join on the condition that they could list all telehealth services, not only abortion; since several were still using improvised “fake telehealth centers” and wanted a clear, virtual-only model. We broadened to include STI evaluation and services, birth control, and gender-affirming hormone therapy with six additional affiliates across four states. Due to the rapid iteration and scaling of services, usability testing was skipped for this phase, but we continued to leverage the workshops to validate new design iterations.
Phase 3 – repeatable onboarding at scale. We scaled the stabilized product, offering all interested affiliates the ability to create VHCs within their operating states. Workshops were not used for this phase, but we continued to observe user feedback through usability testing.
Before Phase 1, we learned that several affiliates had created “fake health centers” to route patients to telehealth appointments and work around scheduling-software limitations. These pages appeared to offer telehealth care but were indexed by search engines as physical locations. Because the system required a street address – and displayed it to users – patients were often unsure whether the site represented a physical clinic or a telehealth service. Internally, it appeared we had more physical health centers than we actually did. Before the Dobbs ruling, we counted about three of these improved listings. After the federal abortion protection was removed, the verified ‘fake health centers’ were closer to six. While we didn’t include these initial groups of affiliates in the pilot, the crisis exposed how dire the need was to evolve our digital tools.
Given the urgency for direct-to-patient medication abortion (DTP MAB), we launched the initial pilot in late 2022 with two Midwestern affiliates – one in Illinois and one in Missouri – both offering DTP MAB. These locations served a central corridor where patients frequently traveled 300+ miles for care. As word spread, more affiliates expressed interest. Guided by the organizational-theory concept of tact, we prioritized affiliates already providing DTP MAB so we could address the most critical, time-sensitive need. Although the earliest “fake health center” innovators were not in the first pilot, they joined in Phases two and three.
We invoked tact early on, entering with humility. We framed affiliate workarounds as “field expertise,” not deviations, which opened doors to candid discussion. We chose our words carefully, translating insights into throughput, safety, and staff burden – not just UX language – so clinical and operations leaders could act. And finally, we made sure to close the loop. Each release and version shipped with release notes and affiliate-wide communications that highlighted “what you told us / what we changed” to participating teams, building trust and participation over time. Tact, in this sense, was procedural: a way of sequencing inquiry, framing risks, and sharing credit that made adoption possible across a federated system.
Workshops
PPFA’s prominence required a pilot that could be tested and proven. Workshops were only used for feedback during Phase one and Phase two. Following software-product practice, we launched a minimum viable product (MVP) with two Midwest affiliates (Illinois and Missouri) willing to trial the concept and join our initial launch.
We combined rapid ethnography – increasingly used in health care under complex constraints – with user-research methods from the software industry. Rapid ethnography enables immersive, time-sensitive learning without the full academic guardrails or stringent study designs and has supported operational improvements in other clinical contexts like the COVID-19 surge (Vindrola-Padros and Vindrola-Padros 2018). While scholars debate the depth of short-term studies, evidence shows that focused fieldwork can surface critical insights, especially from less-powerful voices. Cupit and MacKintosh note that what may be most important to time spent ‘in the field’ is the ability to achieve immersion in the setting and engage with ‘less powerful voices’ to gain understanding. Pink and Morgan analyze the differences between intense, anthropological studies and theoretical but short-term ethnographies, and alternative approaches that use the ethnographic label but fail to produce ‘distinctly anthropological ways of understanding’ (Cupit, Mackintosh, and Armstrong 2018). Despite the debate, our team was in crisis, and these approaches were necessary to understand our users quickly and responsibly.
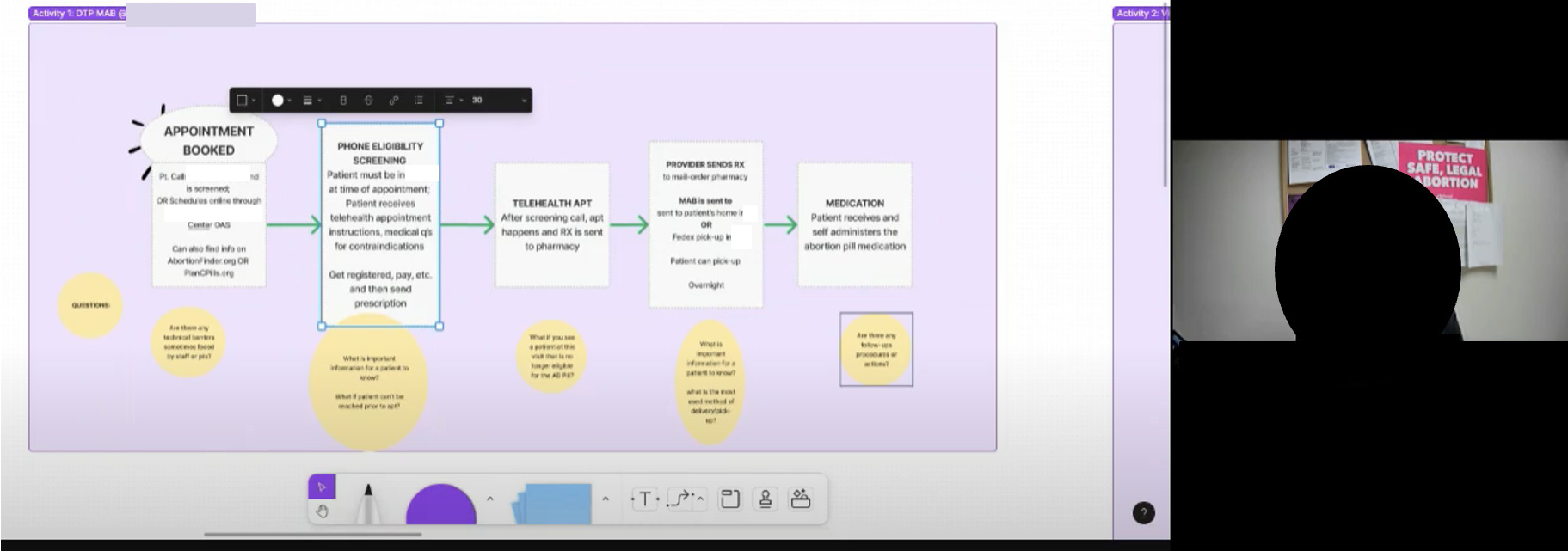
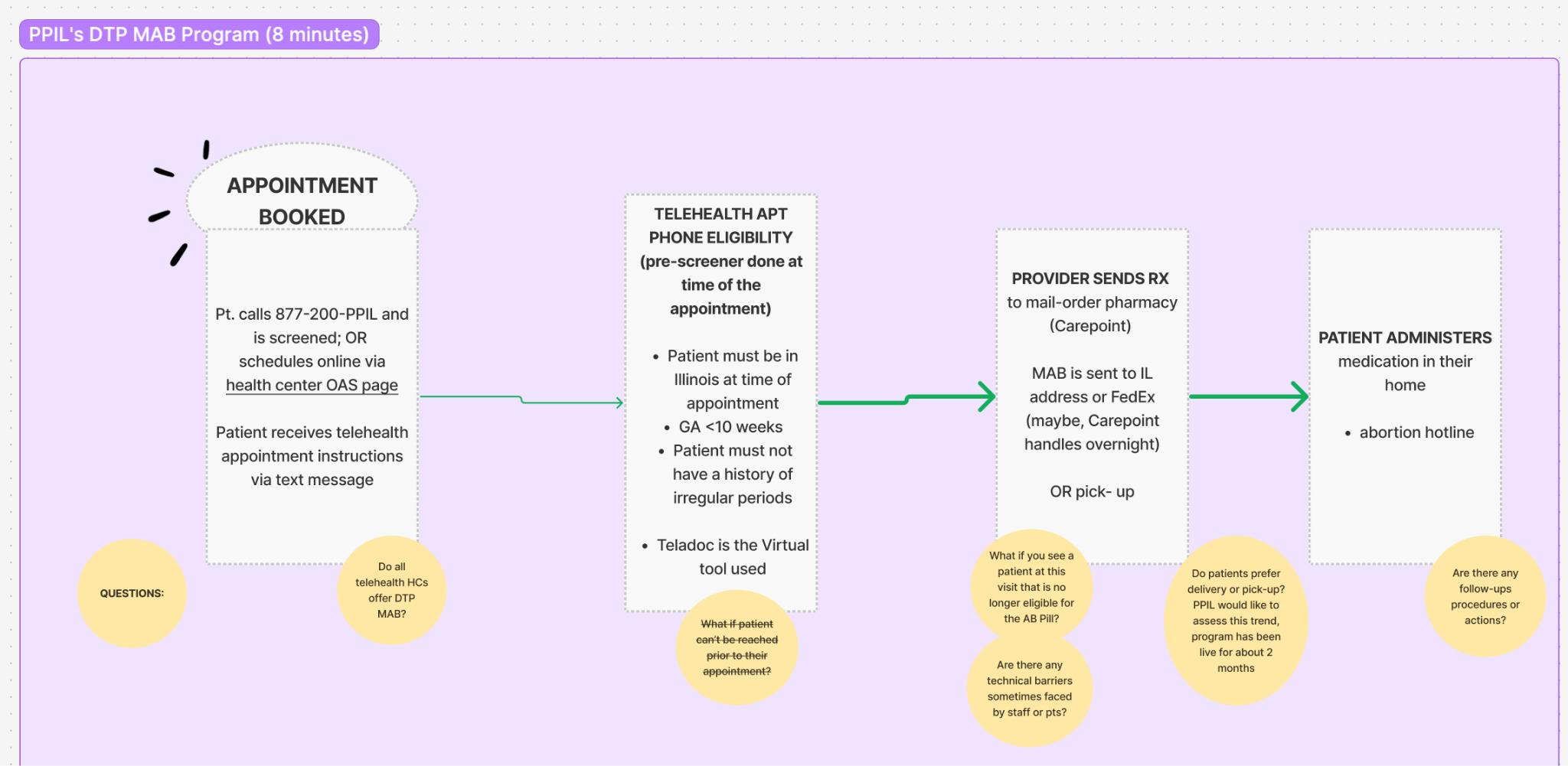
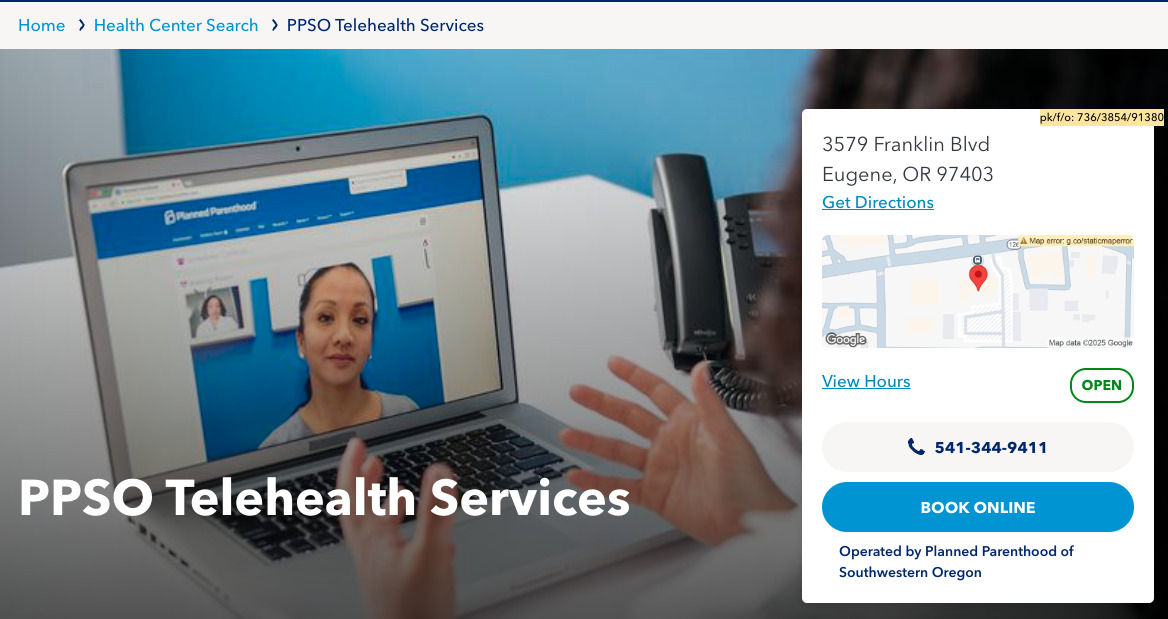
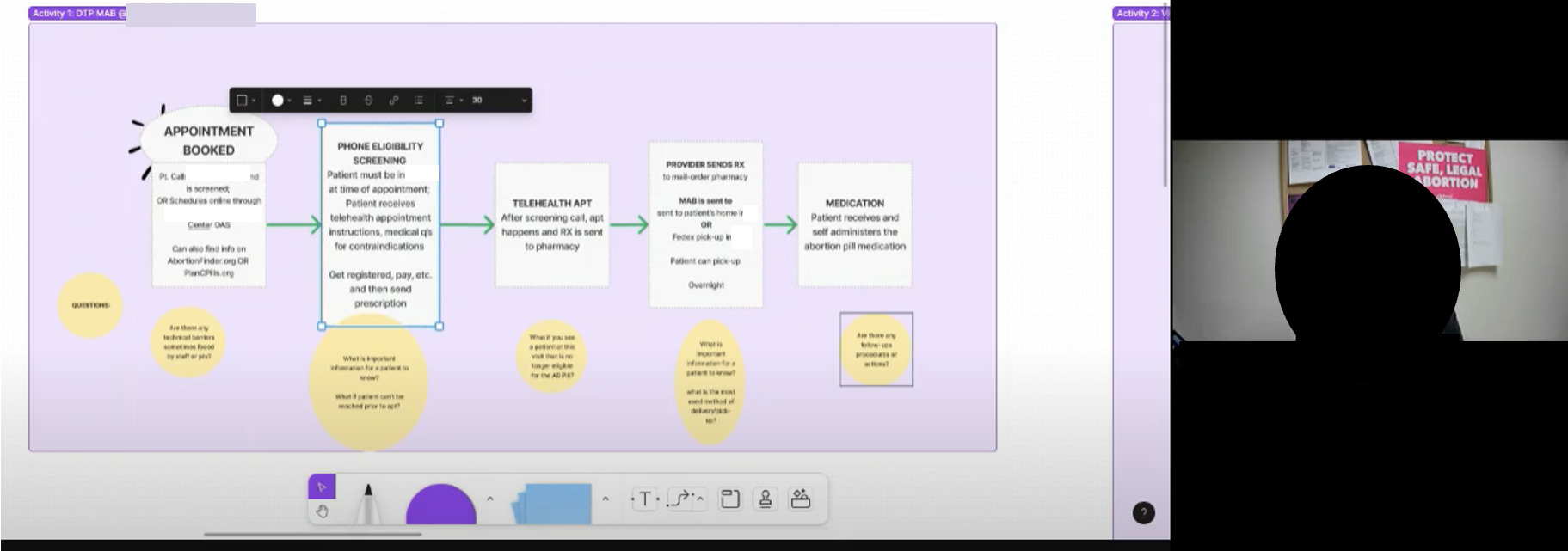
Because of geographic dispersion, we held virtual workshops where providers simulated patient and staff workflows and helped validate design decisions (Fig. 2). Affiliate A and affiliate B were engaged early; their in-clinic practices anchored our vision so VHCs would work for real operational needs. Nurse practitioners and web administrators directly involved in DTP MAB mapped end-to-end processes, systems, and touchpoints before and after the visit. This surfaced gaps and opportunities in abortion telehealth and reinforced a broader lesson from complex initiatives (Fig. 3): creativity and inclusiveness drive equitable, effective solutions.
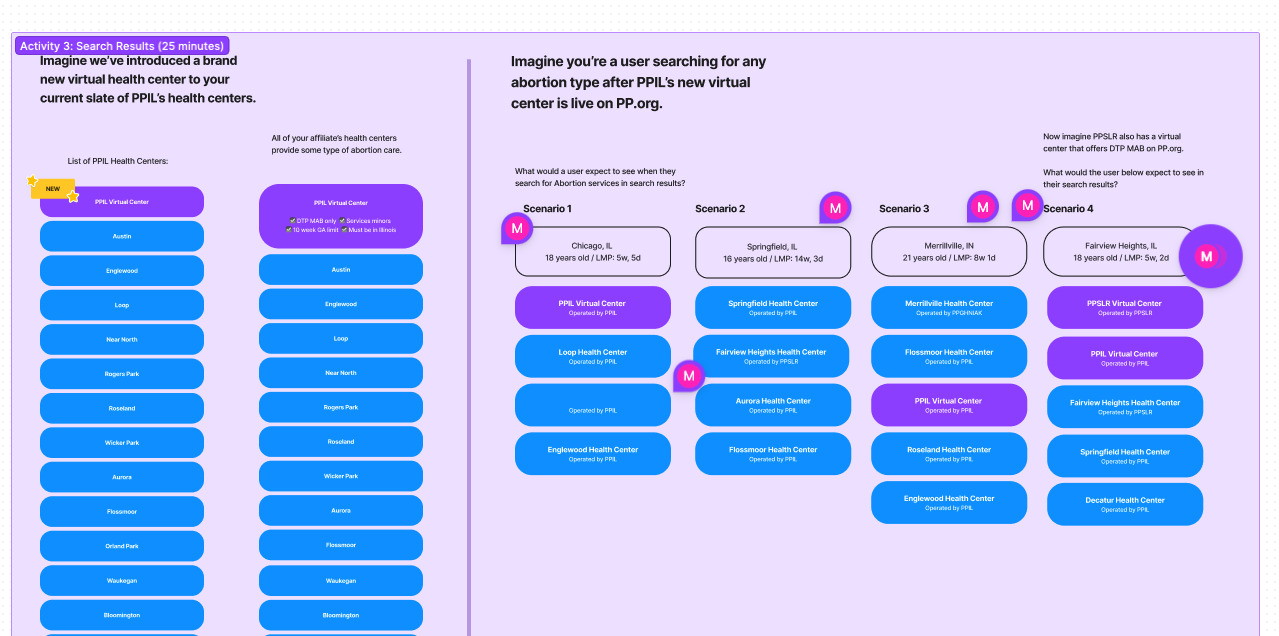
Findings varied by affiliate and informed key product logic. We established how VHC listings should display based on user location, and we defined zip-code management for cases where a search occurred outside a local affiliate’s operating area. Some affiliates expressed interest in sharing telehealth schedules within the same state. We ultimately did not pursue that path, but it underscored a key constraint of our federated structure: layered approvals and state-by-state rules can create friction in getting care and hinder innovation.
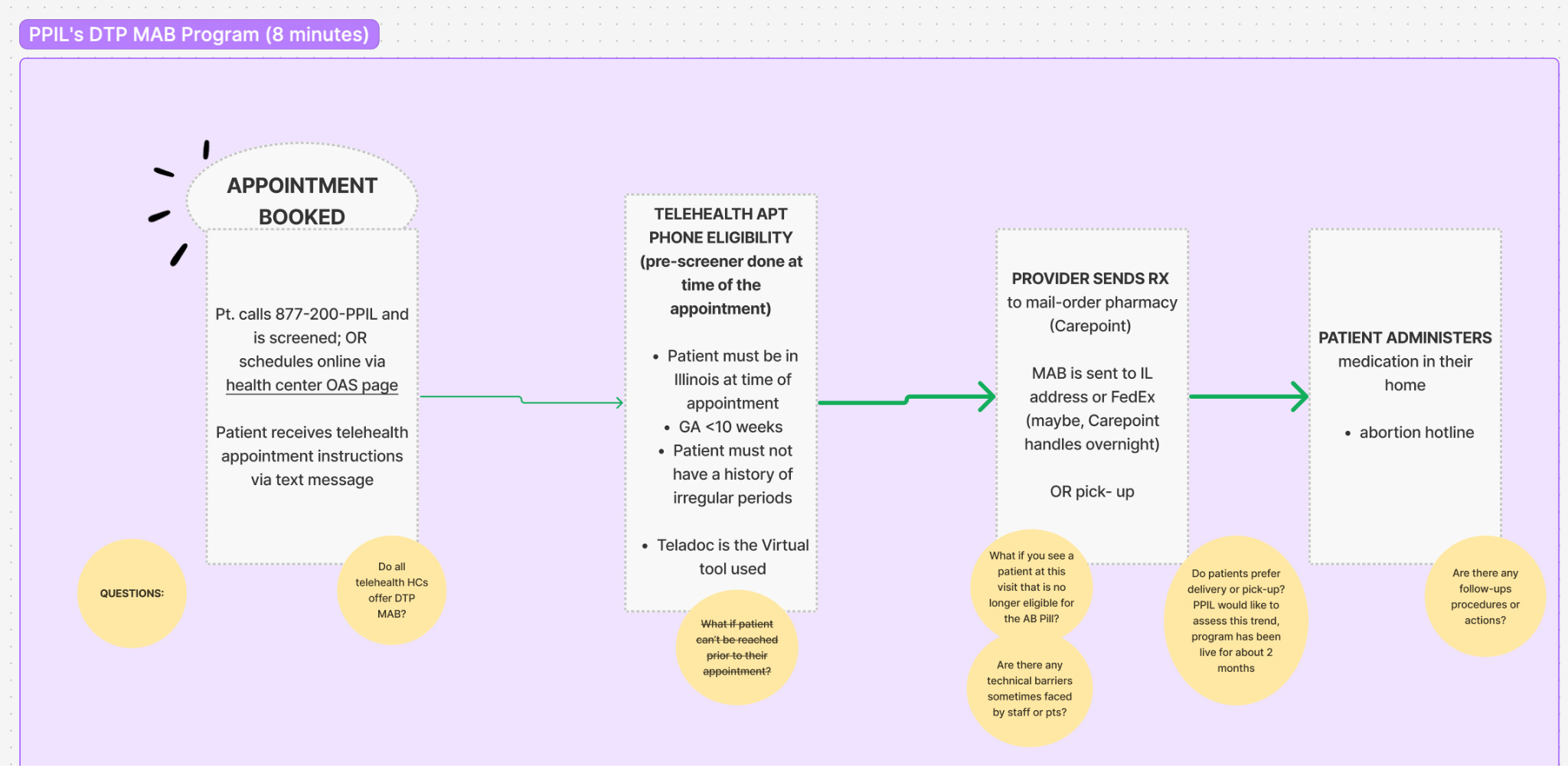
Following the workshops, we produced low-fidelity prototypes for affiliate feedback and conducted usability testing. Usability tests simulate realistic scenarios, while users are asked to complete tasks, and think aloud on what they see to support iterating on the design with each round of input. These workshops proved essential, mirroring evidence from other complex initiatives, where creativity and inclusiveness were key to equitable solutions (Eidenskog, Andersson, and Glad 2024). They welcomed the efforts by our team and provided us with ample time and feedback during and after the workshops. Virtual workshops allowed us to capture and validate patient and provider workflows, highlighting both gaps and opportunities in the abortion telehealth process (Fig. 4). Workshops were interactive, allowing providers and product leads to map out the existing process, systems, and touchpoints before and after the visit.
Most important, the workshops helped define scope and secure buy-in. Internally, some stakeholders resisted a phased approach, arguing for “all services or nothing.” While piecemeal rollout was accepted within the initial pilot, expansion called for more options. Demonstrating early wins while preserving a coherent long-term vision was critical to sustaining momentum and expanding the telehealth program.
Usability Testing
To support the workshops, we conducted moderated usability tests with Spanish- and English-speaking participants on both live pages and proposed designs. Usability testing was conducted during phase one and phase three. Sessions followed real navigation paths and revealed persistent misunderstandings about how telehealth abortion care works. Many participants did not initially realize that medication abortion (pills by mail, where eligible) was available; surfacing this information earlier reduced search time and eased stress during an already emotional moment.
“I wish I had more information on how telehealth works for certain items such as birth control. Will it be shipped to me? For abortion, will an appointment be made on the telehealth visit?”
—Research Participant in Usability Test
We learned that telehealth was the dominant mental model for virtual care, yet our signaling was uneven. Twelve of 13 participants used the term “telehealth” and recognized a VHC as a virtual-only listing. Participants often equated an end-to-end digital flow with “telehealth,” so when online booking was disabled for a brick-and-mortar site, they assumed virtual visits were not offered there. Iconography also created confusion: the pill-shaped “virtual visit available” icon was frequently interpreted as a video-play button, obscuring whether a visit was truly available. At the same time, the VHC detail page design largely worked. Participants praised the three-step “How it works” banner, the tabbed layout, and the real-time hours indicator. Most felt confident booking from this page, though some wanted up-front confirmation on insurance acceptance and clearer guidance on what happens after booking. One participant asked for an explicit phone or chat fallback.
In response, we replaced the pill-shaped icon with a text badge and supporting microcopy to indicate telehealth availability (Fig. 5). We also decoupled availability signaling from booking toggles so that telehealth remains clearly indicated even when online booking is off for a physical site. To address comprehension gaps, we pulled forward eligibility and fulfillment details – such as shipping or dispensing for birth control and medication abortion where applicable – and added a concise “what happens next” explainer. We also included up-front insurance and payment information and ensured a visible phone or chat fallback at key decision points.
_versus_final_design_(right)__iteration_of_a_vhc.png)
Virtual health centers showed early indicators of success, but effectiveness depended on pairing VHCs with online scheduling to drive bookings and reduce no-shows. At affiliate B (Table 1), the pilot produced an increase in kept appointments and a decrease in no-shows. According to Google Analytics, 100% of affiliate B’s DTP MAB online appointments booked during the pilot were via the VHC, indicating that users clearly understood the offering from VHC listings.
Results at affiliate A were inconclusive. Long lead times[3] and a two-month period during which online scheduling was disabled likely contributed to negative outcomes.
The Messy Bits: Operational Lessons
Operational heterogeneity and the federated model. VHCs operate across diverse local contexts – zip-code patterns, pharmacy access, call-center capacity, screening requirements, credentialing, and search engine optimization (SEO). Nurse practitioners and appointment managers remained essential to validating end-to-end workflows. Early improvised solutions —“fake health centers” – worked locally but produced contradictory signals at scale (e.g., indexing as physical sites). Digital product managers formalized these hacks into trusted VHC models, but evolving and scaling the model across independent teams demanded ongoing communication and tact. Solution: Make variability governable with tangible artifacts – clear owners, definitions of “done,” release notes, and concise best-practice guides – so digital processes can be observed, improved, scaled, and sustained across affiliates.
Geography and cross-border routing. While we worked within the legal processes and preferences of each affiliate, patients often crossed state lines while eligibility, licensing, and fulfillment rules changed at the border. PPFA’s “areas of service,” or geographic coverage areas, are operated by different affiliates with distinct tools and processes. Listing logic, availability, and routing required continual reconciliation to prevent misdirection. Solution: Centralize routing rules and maintain a single source of truth for geography and service eligibility to minimize drift and reduce corrective workload.
Information architecture (IA) and patient comprehension. Users struggled to find care across borders and often interpreted “no online booking” as “no telehealth.” They also missed virtual options nested under brick-and-mortar listings. Solution: Validate the IA with targeted studies; favor clear labels and cross-links; keep telehealth availability visible even when booking is off; provide explicit “what happens next” guidance and phone/chat fallbacks to improve findability and confidence.
Scheduling in sync with Online Appointment Scheduling (OAS). Launch risk rises when systems do not match (the national website and OAS tool). Patients hit dead ends or get pushed to call, which erodes trust and adds work for staff. Solution: Don’t go live until the website and OAS are in sync. Use OAS as the single source for what services and times are truly available and treat it as the source of truth for availability and routing to protect conversion.
Onboarding readiness and a defined path to completion. The most acute early pain point was telehealth scheduling setup: teams were unsure whom to contact, the required hand-offs, or what “complete” looked like. Solution: Allocate sufficient lead time and establish a single accountable owner, a documented checklist, environment hand-offs, and target timelines to reduce rework and accelerate time-to-live.
Where VHCs Are Today
As of September 2025, 44 Virtual Health Centers operate across 37 states, supported by 27 affiliates. The breadth of services, listed by highest volume of appointments, includes: birth control, medication abortion (where eligible), gender-affirming care, STI evaluation and treatment, pain and inflammation care, emergency contraception, PrEP and PEP, and menopause care. Core flows run in Spanish and English, and cross-affiliate staffing increasingly extends service hours beyond local clinic schedules.
To date, patients have booked close to 300K appointments through VHCs. No-show and cancellation rates remain at or below brick-and-mortar benchmarks. A mixed-methods approach – using pre and post appointment data paired with qualitative feedback, plus heatmaps, A/B tests, and analytics – guided iterative design changes, balancing measurable gains with human-centered improvements.
Operationally, the product is more mature and predictable. OAS parity at launch is enforced via a readiness checklist covering services, naming conventions, a single-path onboarding flow with defined roles, eligibility logic, and insurance/payment disclosures. Content and user experience governance standardize labels and information architecture across affiliates, while shared dashboards and regular reviews sustain a common performance view. Together, these practices enable VHCs to meet patient expectations while satisfying clinical and legal requirements.
Impact and Final Takeaways
Crisis as catalyst. Crisis compresses decision cycles and surfaces urgent needs. Progress often requires relaxing legacy protocols rather than waiting for perfect alignment or prescriptive guidance. In these conditions, rapid ethnography is both appropriate and effective; it turns frontline observation into actionable changes in practice and policy.
Tactful framing and staged delivery enable adoption. In a federated system, adoption hinges on how change is explained and paced. Translate user insights into operational terms (throughput, safety, staff burden), assign clear owners, and sequence releases with explicit “what you told us / what we changed” loops. Workshops set scope and secured buy-in amid “all services or nothing” objections. Narrow pilots, early wins, and a visible path to full-service telehealth turned initial resistance into durable adoption.
Workarounds are demand signals. Staff improvisations reveal unmet needs faster than instrumentation alone. Treat workarounds as prototypes: document them, test the underlying intent, and formalize them into first-class product patterns. This complements algorithmic approaches, which may miss local constraints and human context.
About the Authors
Monica Diaz McMillan is Associate Director, Planned Parenthood Federation of America. She is a digital product leader and trained sociologist and anthropologist with deep experience driving mission-driven technology across startups, nonprofits, government, and health care. As Associate Director at Planned Parenthood Federation of America, she applies agile methodologies, ethnographic research, and human-centered design to deliver scalable, user-first solutions in sexual and reproductive health. With over 15 years of experience, her portfolio spans clinical software, public health tools, and community health systems, as well as consumer products for brands like Sephora, Estee Lauder, Samsung, Coach, AXA Equitable, and Blue Cross Blue Shield. Grounded in social justice and health equity, Monica also guides healing journeys through music and integrative practices.
Carolina Treviño is Associate Director, Planned Parenthood Federation of America. She is a Brooklyn-based product manager with eight years of experience leading cross-functional teams to design and deliver mission-driven digital products. She has collaborated with organizations such as the Ad Council, Power the Polls, and The Learning Network to create impactful user experiences that drive positive change. Currently serving as the Associate Director of Product Management at Planned Parenthood, she oversees key initiatives focused on patients searching for care, abortion patient wayfinding, and comprehensive sexual and reproductive health education.
Alan Necula is a technical product manager with 20+ years of experience in software development, product management, and leading development and product teams. He has led mission critical digital initiatives related to fundraising, online appointment scheduling, and data integrity. Alan lives and works in Brooklyn, New York alongside two beloved cats.
Brianna Martinez is Senior Digital Product Designer, Planned Parenthood Federation of America. Based in Portland, she has over a decade of experience in UX and brand design. She started her career in the Bay Area and now brings a human-centered/user-first approach to the work at Planned Parenthood, where she aims to make digital products useful and accessible. She is especially interested in the intersection of design, psychology, and human behavior.
Disclosures
All participating names of affiliates were anonymized for privacy reasons.
Legal navigation: we worked within the legal state processes and unique affiliate preferences of each state to define each condition and list what was appropriate to display for patients and affiliates. We considered state lines, licensing, and telehealth and medication dispensing rules across state borders.
All authors are, or previously were, employees of Planned Parenthood Federation of America and all relevant regulatory and legal requirements were adhered to in performance of this research.
Notes
A resounding thanks to our editors and advisors: Camille Kramer Courbariaux, Andreas Wester, Robert McMillan, Nadia Haque.
Special thanks to the Digital Monsters scrum team, and all the supporting staff across PPFA who contributed to making the program and this case study a success: Yolanda Matthews, Heather Bendix, Amy Bryant, Tyler Kershner, Juan Jimenez, Kevin Williams, Claire Choate, Christina Langoria, Elise Gust, Fatima Hassan, John DuPre, Lemonia Stroubos, Madhavi Gadipally, Marcela Uribe, Matt Goins, Megan Shea, Michael O’Keefe, Michael Smallwood, Milan Aljetic, Miloš Nikić, Naily Nevarez, Nicole Levitz, Nina Hessell, Rachael Lacey, Rosette K. Diaz, Veronica Blackwell
Planned Parenthood Federation of America is a nonprofit organization providing low-cost reproductive, sexual health, and family planning medical services through clinics across the United States. It was founded in 1916 and supports close to 45 affiliate individual non-profit healthcare organizations associated with the PPFA brand. Collectively, affiliates operate over 500 physical and virtual health centers across the country.
Lead time at PPFA is the number of days before an appointment time is available for booking. The more days there are before the appointment, the more likely a patient will not show or cancel.
WeCount is a time-limited reporting effort led by the Society for Family Planning that aims to capture national shifts in abortion volume, by state and month, following the Dobbs v. Jackson Women’s Health Organization Supreme Court decision to overturn Roe v. Wade. This report includes data from April 2022 to December 2024. https://societyfp.org/research/wecount/wecount-december-2024-data/#:~:text=The%20monthly%20number%20of%20abortions,the%20end%20of%20December%202024